Understanding TreatmentOptions in
Cutaneous Lymphoma
6
7
Cutaneous T-Cell Lymphomas
2
DiseaseClassification/Staging
CTCLs are classified into stages IA through IVB using theT (tumor,which
forCTCL is patches or plaques),N (lymphnode),M (presence ofmetastasis)
(TNM) system.
2
The level of disease is evaluated based on the size of the
plaques or patches of affected skin (T1–T4); the presence or number of cancer
cells in lymphnodes (N0–N3); and the presence ofmetastasis (M0–M1) (
Table
2
). Stages IA, IB, and IIA are considered early-stage disease,meaning that the
cancer is not widespread. Stages IIB through IVB are considered advanced-
stage disease,where the cancer ismorewidespread and/or hasmoved outside
the skin to other places in the body such as the lymphnodes or other organs.
Sincemycosis fungoides andSézary syndrome include involvement of the
blood, staging of these cutaneous lymphomas includes this additional criteria
based on the presence of Sézary cells in the blood.
2
B
0
represents an absence of
significant blood involvement,B
1
represents a low blood tumor burden, andB
2
represents a high blood tumor burden.
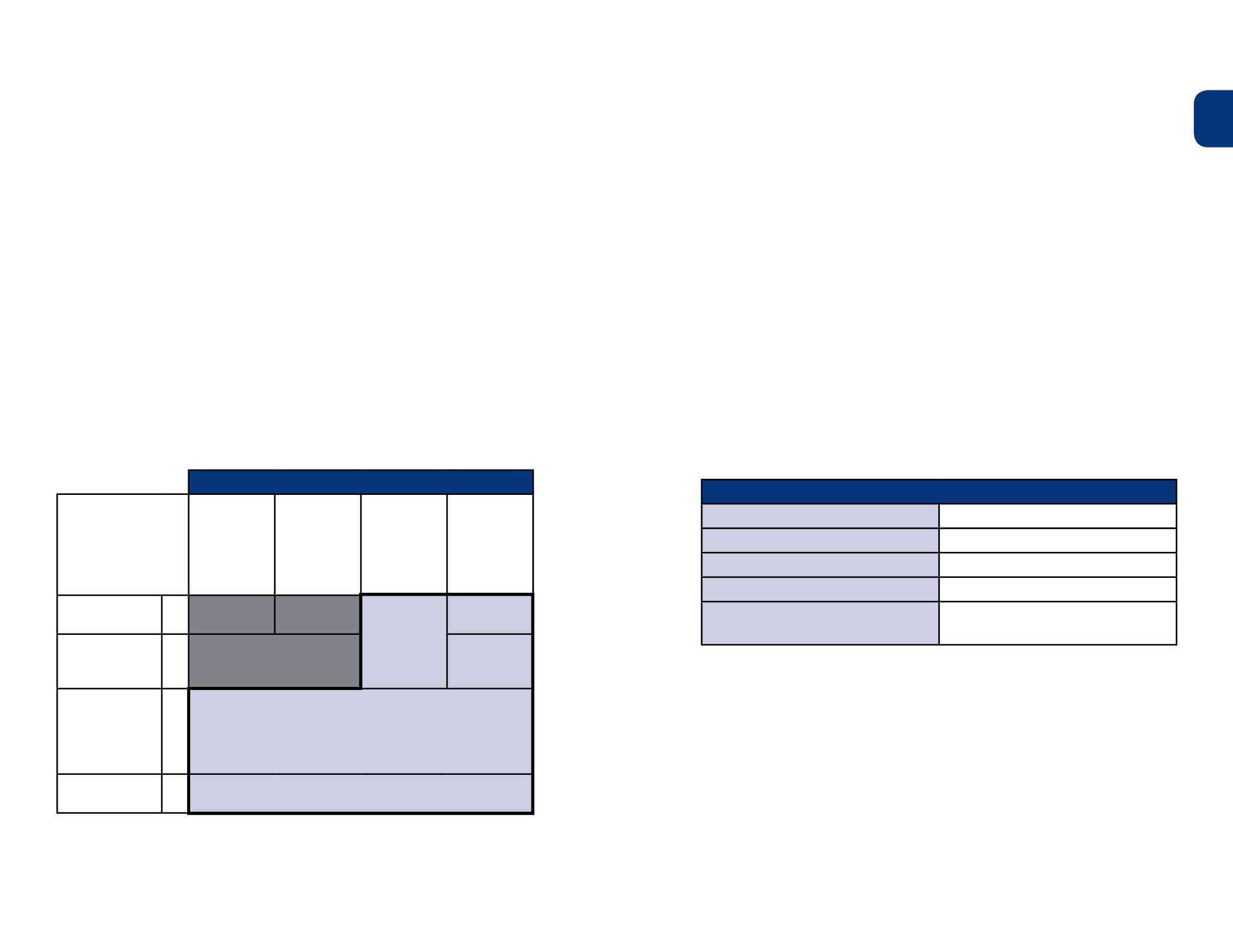
Table2.
Staging ofCTCLs by theTNMSystem
a
a
The grey-shaded regions indicate early-stage disease,whereas the blue-shaded areas indicate
advanceddisease.
2
BSA, body surface area.
TreatmentOptions
PatientswithCTCLwhohave early-stage disease can be treated effectively
with skin-directed therapies.
3
Skin-directed treatments forCTCL include
topical therapies like topical steroids, phototherapy, and radiation.Topical
treatments are applied to the skindirectly and aremostly active on the surface
of the skin,withoutmuch absorption into the bloodstream.This can limit
side effects.Patients can often use skin-directed therapies for a long time.
4,5
Although the diseasewill probably come back (relapse), the same treatment that
workedpreviously oftenworks again. Skin-directed therapies are recommended
alone or in combination for treatingmycosis fungoides and other early-stage
CTCLs (
Figure1
).
For patientswith large areas of skin involvement or lymphoma that has spread
beyond the skin or has relapsed, systemic therapies that canmove through
the bloodstream and extend throughout the entire body to reach cancer cells
wherever they are located, such as oral retinoids, interferon, or extracorporeal
photopheresis,might be used early on in combinationwith skin-directed
treatments,
6,7
depending on the individual patient’s clinical circumstances.
a
This list shouldnot be considered exhaustive.Patients andphysiciansmay decide on other
combinations that are appropriate for their particular situation.
TheNational ComprehensiveCancerNetwork® (NCCN®;www.nccn.org),
a not-for-profit alliance of 25 of theworld’s leading cancer centers, develops
guidelines on the treatment of cancers including cutaneous lymphoma.An
overview of theNCCNCTCL guidelines are shown in
Figure1
.
5
Tumor (T)
Lymphnodes (N)
Metastasispresent (M)
T1:
Limited
patches/plaques
(<10%BSA)
T2:
Generalized
patches/plaques
limited to 1 or 2
contiguous body
regions (
≥
10%
BSA)
T3:
Generalized
skin
involvement, or
1–2 tumors
≥
1 cm in
diameter
T4:
≥
80% of
BSA affected
N0:
Nonodes are
clinically involved
M0
IA
IB
IIB
IIIA
N1:
Nodes enlarged,
histologically
uninvolved
M0
IIA
IIIB
N2-3:
Nodes
clinically normal
(N2) or enlarged
(N3), histologically
involved
M0
IVA
N0-3:
Visceral
involvement
M1
IVB
CommonCombination Therapies
a
Skin-directed+Systemic
Systemic+Systemic
Phototherapy + retinoid
Retinoid + interferon
Phototherapy + interferon
Photopheresis + retinoid
Phototherapy + photopheresis
Photopheresis + interferon
Total skin electron beam +
photopheresis
Photopheresis + retinoid + interferon


